


REVIEWS
Dilated cardiomyopathy (DCM) is an etiologically heterogeneous myocardial disease with a prevalence of up to 1:250 and is associated with mutations in more than 100 genes. However, pathogenic variants are identified in only 30–40% of cases. This review systematizes current data on the genetic landscape of DCM. According to international criteria, only 12 genes (including LMNA, TTN, MYH7, SCN5A, RBM20, DSP, FLNC) have a high level of evidence, whereas the majority of commercial gene panels include genes with minimal supporting data. In addition to monogenic forms, single nucleotide polymorphisms (SNPs) in genes such as IL-32, CD247, MMP2, MBL2, and components of the renin-angiotensin-aldosterone system (RAAS) play a significant role by modulating disease risk through the regulation of inflammation and extracellular matrix remodeling. The clinical significance of genetic testing lies in its ability to stratify the risk of sudden cardiac death (especially in the presence of mutations in LMNA, RBM20, FLNC) and to develop personalized therapeutic approaches. Thus, genetic testing is becoming an indispensable tool in modern cardiology. The search for literary sources was carried out in scientific databases PubMed (https://pubmed.ncbi.nlm. nih.gov/), eLIBRARY.RU (https://elibrary.ru/), Embase (embase.com), Web of science (https://www.webofscience.com), Google Scholar (scholar.google.com) for the period 2005–2025.
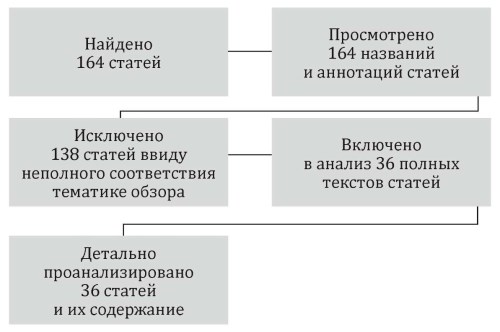
There has long been a need to systematize the extragastric manifestations of gastritis, similar to the extraesophageal manifestations of gastroesophageal reflux disease. In this descriptive review, the authors attempt to determine the feasibility of grouping extragastric lesions in Helicobacter pylori-associated gastritis, which may be related by etiologic or pathogenetic principles. Particular attention is paid to the impact of comorbidities on the patient’s body, the difficulties of diagnosing coinfections, determining the role of each, and the effectiveness of treatment for numerous extragastric manifestations. Literature sources were selected from PubMed and the Russian Science Citation Index (RSCI). Initially, 164 scientific articles were identified based on titles and abstracts. Thirty-six articles were selected for detailed analysis.
This article presents an analysis of the clinical, neurophysiological, and neuroimaging features of mild to moderate cognitive impairment (CI) in vascular cognitiva disorders. The relevance of the study is due to the high prevalence of cognitive disorders of vascular origin, their significant impact on patients’ quality of life, and the need for their early and accurate diagnosis. The analysis is based on data from clinical scales, ultrasound duplex scanning of the brachiocephalic arteries, and magnetic resonance imaging (MRI) of the brain. Key markers of vascular and neurodegenerative damage were assessed, including the degree of arterial stenosis and occlusion, characteristics of atherosclerotic plaques, as well as neuroimaging signs such as leukoaraiosis, lacunar infarcts, brain tissue atrophy, and microbleeds. It is shown that the diagnosis of CI requires a comprehensive approach, in which the leading role is given to the objective assessment of cognitive functions using standardized scales and questionnaires. The most informative screening tools in clinical practice are the MoCA and Mini-Cog scales, which can detect both moderate and more pronounced cognitive impairments. The combined use of neuropsychological testing and neuroimaging methods improves diagnostic accuracy, helps clarify the origin of the cognitive deficit, and determines further patient management strategies.
ORIGINAL RESEARCH
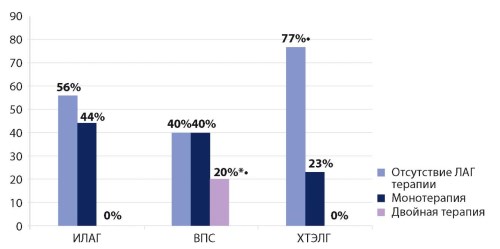
Objective: to evaluate the characteristics of PAH-specific and symptomatic therapy, treatment escalation dynamics, and the incidence of adverse events over a 3-year follow-up period in patients with pulmonary hypertension (PH) of various etiologies. Materials and methods: the study included patients with PH of different etiologies: idiopathic pulmonary arterial hypertension (IPAH, n=30), PH associated with congenital heart disease (CHD, n=30), and chronic thromboembolic pulmonary hypertension (CTEPH, n=31). We analyzed the duration and structure of PAH-specific therapy, as well as the incidence of adverse events. Statistical analysis was performed to assess intergroup and pairwise differences, which were considered statistically significant at p < 0.05. Results: Results: analysis of PAH-specific therapy at baseline revealed that prior to study enrollment, 77% of patients with CTEPH had not received any PAH-specific therapy, which was significantly more frequent than in the CHD group (p3=0,004). Dual therapy prior to enrollment was more commonly used in patients with CHD (20%), whereas it was absent in the IPAH and CTEPH groups (pmg=0,004). Following therapy escalation, differences regarding the absence of PAH-specific treatment were no longer significant; however, treatment patterns differed: dual therapy remained more frequent in the CHD group (37%; pmg=0,017), sildenafil was more frequently prescribed to patients with CHD (70%; pmg=0,003), and riociguat was more frequently prescribed to patients with CTEPH (55%; pmg <0,001). At the 3-year follow-up, patients with IPAH showed a significant increase in the proportion receiving triple therapy (p2 =0,001; pmg=0,007), patients with CHD showed a decrease in monotherapy and an increase in dual therapy (p2 =0,007 and p2 =0,005, respectively), whereas no significant changes in the structure of PAH-specific therapy were observed in the CTEPH group. Analysis of adverse events revealed the highest 3-year mortality rate in the IPAH group (16%). At 1 year, the composite endpoint (all-cause mortality and >1 hospitalization per year) was more frequently observed in patients with IPAH and CTEPH (pmg=0,004). Conclusion: in patients with IPAH, treatment escalation was characterized by an increase in triple therapy regimens; in CHD-associated PH, by a shift from monotherapy to dual therapy; and in CTEPH, monotherapy with riociguat predominated. These findings support the need for an etiology-specific approach to PH management. Adverse events were more frequently reported in patients with IPAH and CTEPH.
Objective: To perform a comparative assessment of the cardiometabolic profile in young male and female adults over a 10-year prospective follow-up period. Materials and methods: the prospective cohort study enrolled 251 young adults (18–44 years old): 124 males (median age 27 [21–36] years) and 127 females (median age 35 [26–41] years). The assessment included anthropometric parameters, cardiometabolic risk factors, lipid and carbohydrate profiles. Results: males were characterized by higher values of BMI, waist circumference, systolic blood pressure, and a higher frequency of hyperuricemia (OR 4.15; p < 0.05), and the smoking rate increased by 19.8% in men and by 32.7% in women. The prevalence of metabolic syndrome increased, reaching statistical significance in women (from 28.3% to 47.2%; p=0.014), and cases of type 2 diabetes mellitus were registered for the first time (4.8% of men, 2.4% of women). A predictive model for the development of metabolic syndrome was developed, including sex, age, non-HDL cholesterol, leptin, and fibrinogen (AUC=0.911; 95% CI 0.854–0.951). The cut-off value of leptin > 29.1 ng/mL for females (AUC=0.875; sensitivity 78.4%, specificity 87.8%) and non-HDL cholesterol > 3.76 mmol/L for males (AUC=0.798) demonstrated high predictive value. Conclusion: significant gender differences in the cardiometabolic profile of young adults were identified. The developed predictive model with gender-specific cut-off values allows for the identification of a high-risk group for metabolic syndrome development, enabling early prevention strategies.
Objective: to evaluate the characteristics of the daily profile of blood pressure, central aortic pressure, arterial stiffness, and hemodynamic response to simulated psychoemotional stress in patients with arterial hypertension and varying degrees of obesity. Materials and methods: the study included 63 patients (29 with stage I obesity, 34 with stage II) with uncontrolled arterial hypertension. All subjects underwent office blood pressure (BP) measurement, 24-hour BP monitoring ABPM) with assessment of the 24-hour BP profile, central aortic pressure (CAP), and arterial stiffness. Simulated psychoemotional stress (SPS) was carried out using the following mental tests: arithmetic counting according to E. Kraepelin, searching for numbers in K.K. Platonov’s red-and-black table, a task of public reading of an unfamiliar text with critical comments and a time limit if the patient was interested. It was assumed that 3 types of hemodynamic response of systolic BP (SBP) to SPS were distinguished: type 1 — an increase of 5–19 mm Hg. from the initial, type 2 — by 20–39 mm Hg and type 3 — by 40 mm Hg or more. Results: when assessing the parameters of ABPM, CAP, and arterial stiffness in patients depending on the severity of obesity, a relationship was found: individuals with hypertension and stage I obesity had lower values of the studied parameters compared to respondents with stage II obesity. Against the background of SPS, patients with hypertension and stage I obesity most often observed type 1 hemodynamic response (90,5% of cases, respectively), and a small number recorded a decrease in SBP by an average of 5,1 mmHg. In respondents with stage II obesity, compared with the group with stage I, statistically significantly (p < 0,001) more often recorded more pronounced types of hemodynamic response (2 and 3) — 73,5% and 3% of cases, as well as an increase in diastolic blood pressure and heart rate. Conclusion: when assessing the indicators of ABPM, CAP, arterial stiffness and the response of blood pressure and heart rate to SPS, the highest values of the studied parameters and a pronounced hypertensive response were recorded in patients with hypertension and stage II obesity compared to individuals with stage I obesity, which may confirm the greater “stress susceptibility” of this category of respondents.
Objective: to evaluate HRV parameters derived from Holter electrocardiogram monitoring (Holter-ECG) in patients with stable CAD according to the presence of depressive symptoms, and to analyze differences in these parameters depending on the management strategy for CAD. Materials and methods: the study included 89 patients with stable CAD, functional class II–III (n=89), of whom 45 were assigned to a surgical treatment group and 44 to a conservative treatment group. Results: based on psychometric testing results, both groups were further stratified according to the presence or absence of depressive symptoms. Conclusions: the presence of depressive symptoms was associated with reduced rMSSD and pNN50 values. Furthermore, among patients with depressive symptoms, SDNNi and pNN50 parameters were significantly lower in individuals hospitalized for percutaneous coronary intervention (PCI) with stenting compared to those managed conservatively. Depressive symptoms in patients with stable CAD are associated with impaired time-domain HRV parameters, particularly reflecting parasympathetic modulation.
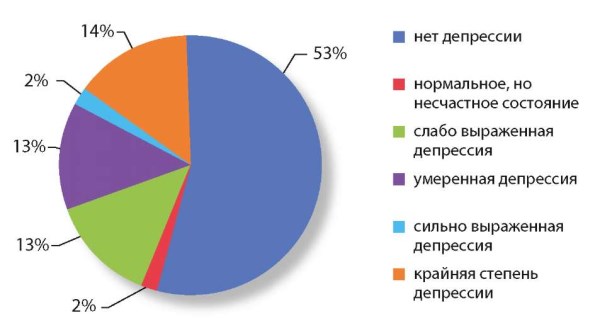
Objective: to evaluate the sensitivity and diagnostic value of commonly used questionnaire methods (SF-36, WHO, Beck Scale, Nottingham Health Profile, CES-D, HADS, Burns Scale) for determining the level of depression, anxiety and quality of life in patients with liver cirrhosis. Materials and methods: the study was conducted using a cross-comparison of questionnaire methods followed by a comparative analysis of the data obtained. Results: it was found that each method has a different sensitivity to the determination of psycho-emotional disorders and quality of life. Conclusion: careful selection of tools is required depending on the specific objectives of the survey.
CLINICAL CASES
Congenital heart disease in the form of a single left ventricle is a rare congenital pathology, the clinical prognosis of which directly depends on timely surgical intervention. In some patients, the anatomical features of the defect balance pulmonary and systemic blood flow, allowing them to survive into adulthood without surgery. This clinical case report aims to present such a patient, who survived to the age of 29, but with an unfavorable outcome due to additional complicating factors.
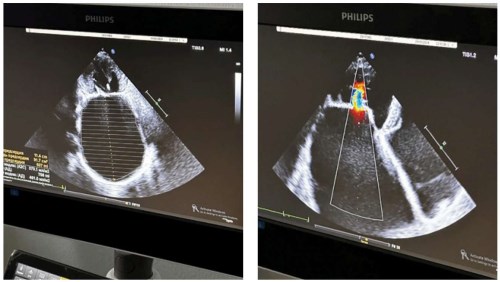
Atriomegaly (giant left atrium (LA)) is a rare but severe complication of long-standing rheumatic heart disease. This condition is associated with a high risk of atrial fibrillation and thromboembolic complications, as well as compression of adjacent structures. We present a case of treatment of a 56-year-old female patient with rheumatic heart disease, combined mitral and aortic valve disease, and formation of a giant LA (volume up to 761 ml, anteroposterior dimension up to 99 mm). The patient underwent simultaneous double valve replacement, tricuspid valve repair, and surgical left atrial reduction. Surgical correction of atriomegaly in combination with valve replacement allows for significant reduction of atrial volume, improvement of hemodynamics, and prevention of fatal complications.
Parathyroid carcinoma is an extremely rare malignant neoplasm of the endocrine system, accounting for less than 1% of all cases of primary hyperparathyroidism. The disease is characterized by pronounced hormonal activity, severe hypercalcemia, and a high risk of target organ damage, which largely determines the severity of its clinical course [4,5]. Due to the absence of specific clinical manifestations and the rarity of this entity, preoperative diagnosis of parathyroid carcinoma remains a significant clinical challenge. This article presents a clinical case of parathyroid carcinoma in a 39-year-old female patient, accompanied by extremely elevated parathyroid hormone levels (up to 1534 pg/mL) and marked hypercalcemia. A distinctive feature of this case was the presence of a large right-sided cervical mass initially interpreted as thyroid pathology, as well as the coexistence of parathyroid carcinoma with autoimmune thyroiditis. The report includes detailed laboratory, imaging, and histopathological findings, outlines the patient’s clinical course, and describes the outcomes of surgical treatment. The presented clinical case highlights the importance of a comprehensive assessment of clinical and laboratory data and emphasizes the need to increase diagnostic vigilance among physicians of various specialties regarding parathyroid carcinoma.
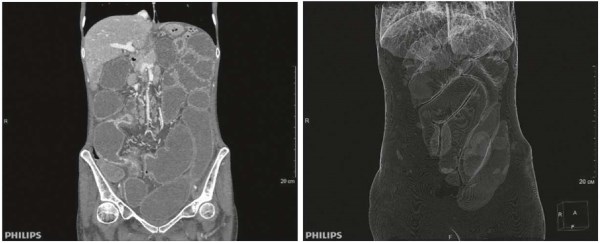
Crohn’s disease often has an aggressive course and leads to severe complications. Often, choosing a surgical or therapeutic treatment approach can be challenging. This article presents a clinical case of a severe course of the stricturing phenotype of Crohn’s disease, complicated by lower subcompensated small bowel obstruction, and discusses the clinical symptoms of the disease and the management approach.

ISSN 3033-8344 (Online)





















